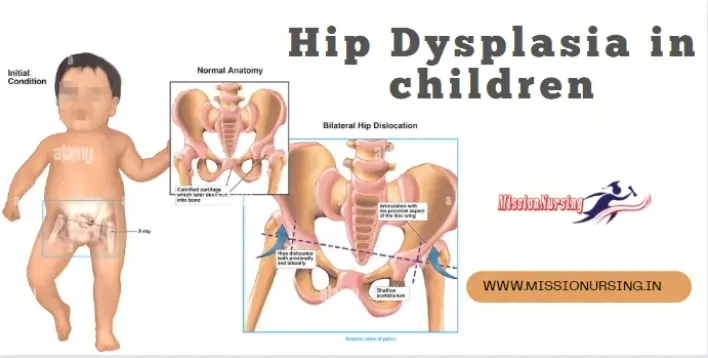
Hip Dysplasia in children Introduction
- Hip Dysplasia is one of the most common congenital malformations in an infant
- Hip dysplasia is defined as the complete and partial displacement of the femoral head from the acetabulum cavity since birth
- Hip dysplasia is a developmental disorder of the Hip, that present in different forms at different ages.
- It may be bilateral or unilateral but If it is unilateral mostly is left hip is affected
Incidence – Hip dysplasia is 1/1000 births
- Hip dysplasia is mainly present in female children (more than 8 times male)
- The left hip is more affected the right hip
Embryonic development of hip
- 4-6 weeks = the hip joints are developed
- 7-8 weeks = acetabulum and head of the femur are develop
- At 11th week = complete development of hip
Risk factors of Hip dysplasia
- A. Genetic – Genetic predisposition, generalized joints laxity, and shallow acetabulum
- B. Hormonal – Maternal relaxing high estrogen so commonly in female
- C. Hip dysplasia is common in 1st born child
- D. Intrauterine malposition – Breach position large baby
- E. Neurological disorder – Cerebral palsy spina bifida
Classification of hip dysplasia
1. Acetabulum dysplasia / preluxation
- Preluxation dysplasia is a mild form of hip dysplasia in which the acetabulum cavity is too shallow or deformed.
- The Head of a female still remains in the acetabulum
- May be chance of hip dislocation later in life
2. Subluxation Hip dysplasia
- Sublucxtion is the most common type of hip dislocation
- Subluxation is known as the Incomplete hip dislocation
- The head of the femur is remaining in the acetabulum cavity but displaced
- The head of femur is partially displaced from its normal position
- Hip is incompletely dislocated due to pressure on the cartilaginous roof of joints .
Luxation / Dislocation
- Luxation is a most severe type of hip dysplasia
- Failed the connect between the head of the femur and acetabulum cavity .
- Completely dislocation of head of femur from the acetabulum
Clinical features of Hip dysplasia
- Features of hip dysplasia at birth or soon after when child start walking
- Birth – Routine screening is suggestive sings in every newborn.
- Early childhood – Asymmetry of groin fold
- Click Limitation of movement
- Older child – Peculiar gait
- No pain
- Limited range of motion of the affected hip
- Asymmetrical abduction in the supine position
- Unequal length of legs
- Abnormality of gait during walking
Clinical signs of hip dysplasia
- 1. Barlow sings – The Barlow maneuver identifies the unstable hip that is in a reduced position that the clinician can passively dislocate.
- If the femoral Head is fail to slip out over the posterior hip of the acetabulum & Immediately slip balk in place when pressure is released is considered a positive Barlow sing .
- 2. Ortolani sing – The done only within 1 month to 3 month The test not done before 1 month or after 3 month of age .
- Ortolani maneuver is performed following Barlow’s test to determine if the hip is actually dislocated
- Apply force will put femur head into the acetebulum & a click sound will be felt
- 3. Positive trendelbarg test – When the child hold in standing position involved leg elevated the pelvis on the dislocated side will be rise
- 4. Allis sing orgaleazzi sing – When the one knee is lower than other
- When the infant is on the balk with the flexed knee dislocation is present this sign.
Diagnosis Hip dysplasia
- History collection and physical examination
- X-ray
- CT-Scan and MRI
- Ultrasound
Management Hip dysplasia
- Treatment of hip dysplasia is to start as soon as because later correction of joints is create more difficulties.
- The main goal of the treatment is the replace the head of a femur within the acetabulum.
Management Hip dysplasia Upto 2 months child (Early Infancy)
- Apply the rigid Device – Friejka pillow or Pavlick harness may be used because these devices permit some movement of the leg.
- To maintain the abduction, use double and triple diapers.
- A closed cell plastic foam pad can be placed with two Diapers to Hold the thigh in position.
- Splint is used last.
Management Hip dysplasia After2-3 months (Late infancy)
- The child is placed in skin traction so that the joints capsule & muscles can be stretched before manipulation of hip joints.
- Skin traction is used in the lower leg (Buck skin traction)
Use spica cast with hip (To maintain the abducted position)
Use splinting Device after the removal of cast
Done the open reduction surgery (Replace the femur Head in acetabulum)
Again spica cast apply after the open reduction for- months.
- Cast should be change in every week up to 6months.
Management Hip dysplasia In older children
- In older children skeletal traction is use.
- Better choice of treatment in older children is open reduction.
- Tenotomy is also affection treatment in older child.
- Cast is apposed after that.
- A nurse assesses the range of motion after remove the cast.
Complications Hip dysplasia
- Failed reduction
- Vascular Necrosis
- Lower back and hip pain
- Premature osteoarthritis of the Hip
- Recurrent subluxation/Dislocation.
- Limb length Discrepancy.
Nursing management Hip dysplasia
- A nurse assesses the newborn for hip dysplasia by physical Examination.
- The nurse Determines the type of hip Dysplasia that occurs in the child.
- Provide the correct position of hip.
- Nurse instructs and Explains to parents about the purpose of using frejka splint or any other Device.
- Nurse educates explain the procedure of how the use splint and keeping the child’s hip in a position of abduction during bathing, Diapering. Etc
- Brace should not be removed in routine care but the bathing brace remove.
- Provide the optimal nutrition and football position use during feeding.
- Care giver should not be use lotions and oil on skin under straps of brace.
- Use the cotton cloths under the brace.
- Change the position of child in 2hourly.
- Encourage the physical, emotional and social development.
- Provide play things which induce movement of upper body.
QnA:-
- Congenital malformation occur when the femur head is dislocated – Hip Dysplasia.
- Hip Dysplasia developmental Disorder commonly affects the – left legs Hip.
- Complete development of hip – At the 11th week of gestational.
- The Head of the femur is still remaining in the acetabulum cavity but the chance of being Dislocated in later life is known – Preluxation Hip Dysplasia.
- The most common type of hip Dysplasia – Subluxation
- Complete hip Dislocation is known as – Subluxation
- The most severe form of hip Dysplasia is – Luxation/Dislocation
- Which device is used to treat hip Dysplasia for a 1month child – Friejka pillow or Pavlick harness?
- Which type of traction is used to treat hip dysplasia in a 3-month child – Skin traction
(Buckskin traction). - Skeletal traction used to treat hip dysplasia in the – Older Children
- A better choice of treatment for hip dysplasia in older children is – Open reduction.